- Постоянный сосудистый доступ для гемодиализа

Содержание
- 2. Основные принципы Успешное лечение ГД возможно только при хорошо функционирующем ПСД. Идеальный доступ: должен позволять канюляцию
- 3. Что это?
- 4. Формировать доступ вовремя! (это не значит - раньше!) Своевременное направление пациента для создания доступа имеет важное
- 5. Не нужно думать, что у нас хуже… Значительные различия между европейскими странами в типе направления и
- 6. Когда формировать доступ? Рекомендуется направление пациентов с хроническим заболеванием почек к нефрологу и / или хирургу
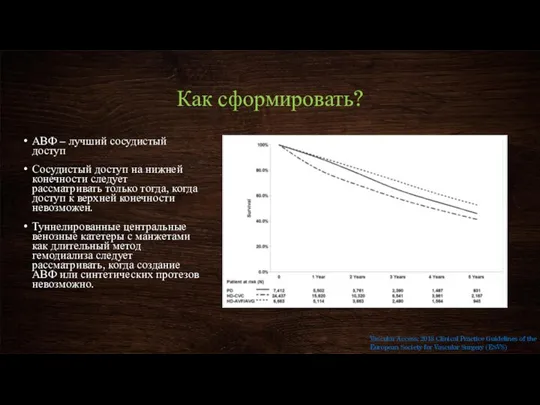
- 7. Как сформировать? АВФ – лучший сосудистый доступ Сосудистый доступ на нижней конечности следует рассматривать только тогда,
- 8. Почему? Причиной создания АВФ является то, что исследования показывают более низкую частоту послеоперационных осложнений и меньшее
- 9. Последовательность создания доступа (идеальная) Принцип венозной консервации диктует, что обычно следует выполнять наиболее дистальную из возможных
- 10. Как облегчить задачу? У пациентов, которые подвергаются или могут нуждаться в гемодиализе, внутривенные инъекции в вены
- 11. Анестезия на операции Региональная анестезия предпочтительнее местной анестезии при операциях на сосудистом доступе из-за возможного улучшения
- 12. Созревание доступа АВФ обычно не могут быть легко использованы после создания, но изменения кровотока приводят к
- 13. Если фистула не созрела? Решение принимается через 6 недель после операции Варианты: Сужение вены – эндоваскулярное
- 14. Пункция доступа Метод «веревочной лестницы» Метод «пункций по площади» Vascular Access: 2018 Clinical Practice Guidelines of
- 15. Пункция доступа Метод «веревочной лестницы» используется вся длина сегмента канюлирования: при каждом сеансе ГД создаются два
- 16. Пункция доступа Метод «пункций по площади» Техника каннюлирования повторно в той же области фистулы. Это приводит
- 17. Катетер длительного стояния Держите повязку в зоне катетера чистой и сухой. Убедитесь, что область введения чистая,
- 18. Катетер длительного стояния Иногда, даже если вы очень осторожны, ваш доступ может закрываться или инфицироваться. Сгустки
- 19. Лечение тромбоза катетера Лечение - это введение лекарственного средства, рассасывающего «сгусток», называемого тканевым активатором плазминогена (tPA).
- 20. Что нужно знать? Знайте свои Kt / V и URR (коэффициент уменьшения мочевины). Kt / V
- 21. Осложнения доступа: инфекции У пациентов с ранней периоперационной ( Раннюю периоперационную ( Seromas are occasional complications
- 22. Осложнения доступа: венозная гипертензия Отек конечности после формирования доступа вероятнее всего связан с сужением центральных вен,
- 24. Скачать презентацию
Основные принципы
Успешное лечение ГД возможно только при хорошо функционирующем ПСД.
Идеальный
Основные принципы
Успешное лечение ГД возможно только при хорошо функционирующем ПСД.
Идеальный
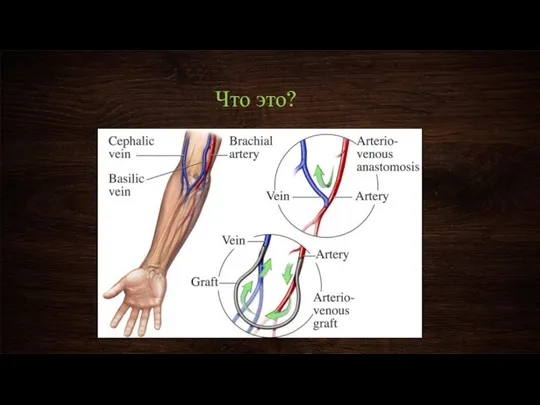
Что это?
Что это?
Формировать доступ вовремя!
(это не значит - раньше!)
Своевременное направление пациента для
Формировать доступ вовремя!
(это не значит - раньше!)
Своевременное направление пациента для
Не нужно думать, что у нас хуже…
Значительные различия между европейскими странами
Не нужно думать, что у нас хуже…
Значительные различия между европейскими странами
Когда формировать доступ?
Рекомендуется направление пациентов с хроническим заболеванием почек к нефрологу
Когда формировать доступ?
Рекомендуется направление пациентов с хроническим заболеванием почек к нефрологу
Как сформировать?
АВФ – лучший сосудистый доступ
Сосудистый доступ на нижней конечности следует
Как сформировать?
АВФ – лучший сосудистый доступ
Сосудистый доступ на нижней конечности следует
Почему?
Причиной создания АВФ является то, что исследования показывают более низкую частоту
Почему?
Причиной создания АВФ является то, что исследования показывают более низкую частоту
Последовательность создания доступа (идеальная)
Принцип венозной консервации диктует, что обычно следует выполнять
Последовательность создания доступа (идеальная)
Принцип венозной консервации диктует, что обычно следует выполнять
Как облегчить задачу?
У пациентов, которые подвергаются или могут нуждаться в гемодиализе,
Как облегчить задачу?
У пациентов, которые подвергаются или могут нуждаться в гемодиализе,
Анестезия на операции
Региональная анестезия предпочтительнее местной анестезии при операциях на сосудистом
Анестезия на операции
Региональная анестезия предпочтительнее местной анестезии при операциях на сосудистом
Созревание доступа
АВФ обычно не могут быть легко использованы после создания, но
Созревание доступа
АВФ обычно не могут быть легко использованы после создания, но
Если фистула не созрела?
Решение принимается через 6 недель после операции
Варианты:
Сужение вены
Если фистула не созрела?
Решение принимается через 6 недель после операции
Варианты:
Сужение вены
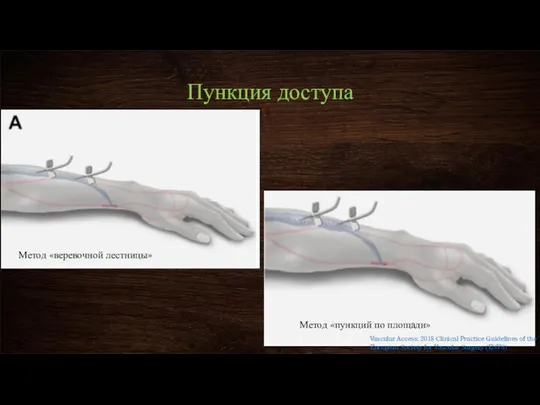
Пункция доступа
Метод «веревочной лестницы»
Метод «пункций по площади»
Vascular Access: 2018 Clinical Practice
Пункция доступа
Метод «веревочной лестницы»
Метод «пункций по площади»
Vascular Access: 2018 Clinical Practice
Пункция доступа
Метод «веревочной лестницы»
используется вся длина сегмента канюлирования: при каждом сеансе
Пункция доступа
Метод «веревочной лестницы»
используется вся длина сегмента канюлирования: при каждом сеансе
Пункция доступа
Метод «пункций по площади»
Техника каннюлирования повторно в той же области
Пункция доступа
Метод «пункций по площади»
Техника каннюлирования повторно в той же области
Катетер длительного стояния
Держите повязку в зоне катетера чистой и сухой.
Убедитесь, что
Катетер длительного стояния
Держите повязку в зоне катетера чистой и сухой.
Убедитесь, что
Катетер длительного стояния
Иногда, даже если вы очень осторожны, ваш доступ может
Катетер длительного стояния
Иногда, даже если вы очень осторожны, ваш доступ может
Лечение тромбоза катетера
Лечение - это введение лекарственного средства, рассасывающего «сгусток», называемого
Лечение тромбоза катетера
Лечение - это введение лекарственного средства, рассасывающего «сгусток», называемого
Что нужно знать?
Знайте свои Kt / V и URR (коэффициент уменьшения
Что нужно знать?
Знайте свои Kt / V и URR (коэффициент уменьшения
Осложнения доступа: инфекции
У пациентов с ранней периоперационной (<30 дней) инфекциейнативной артериовенозной
Осложнения доступа: инфекции
У пациентов с ранней периоперационной (<30 дней) инфекциейнативной артериовенозной
Осложнения доступа: венозная гипертензия
Отек конечности после формирования доступа вероятнее всего связан
Осложнения доступа: венозная гипертензия
Отек конечности после формирования доступа вероятнее всего связан
 Иммунитет. Цитокиновая система
Иммунитет. Цитокиновая система ამოცანების მედიცინა
ამოცანების მედიცინა Клиническая анатомия органов шеи
Клиническая анатомия органов шеи Хроническая болезнь почек (ХБП): Основные принципы скрининга, диагностики, профилактики и подходы к лечению
Хроническая болезнь почек (ХБП): Основные принципы скрининга, диагностики, профилактики и подходы к лечению Зубочелюстные аномалии, принципы их лечения
Зубочелюстные аномалии, принципы их лечения Принципы клинических исследований в создании лекарственных средств
Принципы клинических исследований в создании лекарственных средств Қант диабеті
Қант диабеті Пробиотиктер
Пробиотиктер Физиологические особенности организма дошкольников и младших школьников
Физиологические особенности организма дошкольников и младших школьников Проблемы нечистоплотности кошек и собак. Поведенческий и клинический аспекты
Проблемы нечистоплотности кошек и собак. Поведенческий и клинический аспекты Апаттар медицинасын ұйымдастыру принциптері
Апаттар медицинасын ұйымдастыру принциптері Противосклеротические препараты
Противосклеротические препараты Обучение и воспитание дошкольников с нарушениями слуха
Обучение и воспитание дошкольников с нарушениями слуха Методика исследования готовности старших дошкольников к овладению письмом
Методика исследования готовности старших дошкольников к овладению письмом Навыки взаимодействия с людьми с ОВЗ
Навыки взаимодействия с людьми с ОВЗ Фармакология обезболивающих препаратов
Фармакология обезболивающих препаратов Общая и частная психопатология
Общая и частная психопатология Женское бесплодие
Женское бесплодие L’essayage en prothèse fixée plurale dento-portée
L’essayage en prothèse fixée plurale dento-portée Feeding and Eating Disorders (Расстройства приёма пищи)
Feeding and Eating Disorders (Расстройства приёма пищи) Методы восстановительного лечения в акушерстве и гинекологии
Методы восстановительного лечения в акушерстве и гинекологии ОРВИ. Инфекционные заболевания верхних дыхательных путей,
ОРВИ. Инфекционные заболевания верхних дыхательных путей, Семинар – практикум «Родительская школа: мир на земле начинается дома»
Семинар – практикум «Родительская школа: мир на земле начинается дома» Нейросифилис
Нейросифилис Черепно–мозговая травма
Черепно–мозговая травма Методы исследования в гистологии, цитологии и эмбриологии
Методы исследования в гистологии, цитологии и эмбриологии Анамнестические, клинические и лабораторные особенности впервые диагностированной бронхиальной астмы у детей раннего возраста
Анамнестические, клинические и лабораторные особенности впервые диагностированной бронхиальной астмы у детей раннего возраста Нестероидные противовоспалительные средства (НПВС)
Нестероидные противовоспалительные средства (НПВС)