- Introduction to Psychotic Disorders and Secondary=Organic Psychotic Disorders

Содержание
- 2. מבנה ההרצאה What is Psychosis? Symptoms DDX
- 3. Psychosis Inability to distinguish between the reality and the inner world and stimuli OR- PROFESSIONALLY STATED-
- 5. Why does it happen? Dopaminergic Theory Increasing levels of dopamine in the brain can cause psychosis
- 6. סימפטומים Signs of psychosis Hallucinations Delusions Bizarre or disorganized behavior Impaired thought process Impaired speech output
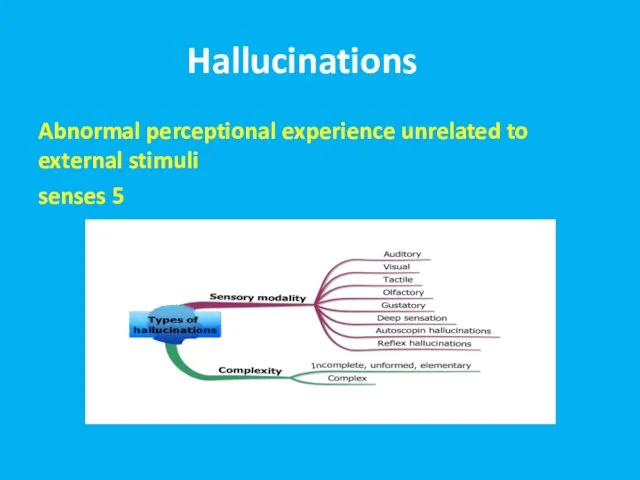
- 7. הזיוHallucinationsת Abnormal perceptional experience unrelated to external stimuli 5 senses
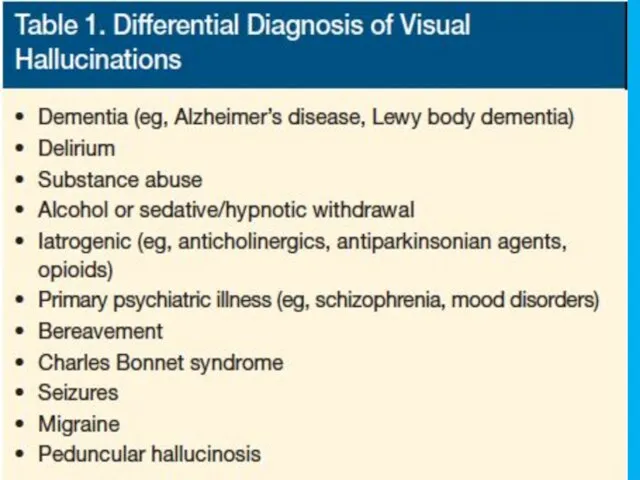
- 8. Reasons for Hallucinations Primary psychiatric disorders Brain pathology Substances Disorders of cranial nerves Delirium Dementia
- 9. Auditory Hallucinations Primary psychotic disorders- human voices, noises, command hallucinations. Usually perceived as coming from outside!
- 10. Taste Hallucinations Usually epilepsy and brain pathology Very rare in primary psychiatric disorders Do not perceive
- 11. Smell Hallucinations Usually epilepsy and brain pathology Rare in primary psychiatric disorders- possible in psychotic depression
- 12. Somatic and Tactile Hallucinations Usually epilepsy and brain pathology In primary psychiatric disorders- possible in delusional
- 13. Visual Hallucinations Usually epilepsy and brain pathology, migraines, visual impairment In primary psychiatric disorders- possible in
- 15. Lhermitte's peduncular hallucinosis Rare neurological disorder Visual hallucinations- vivid, detailed, often moving, exclusively in the dark
- 16. MORE RECENTLY ALSO DIAGNOSED IN PATIENTS WITH MS, FRONTAL AND OCCIPITAL LOBE CHANGES, TEMPORAL ARTERITIS, AND
- 17. Release Hallucinations ANY MODALITY BUT VISUAL MOST COMMON: DEPENDS ON END ORGAN AFFECTED LESIONS ANYWHERE FROM
- 18. Out of Body Experiences Sleep Substances General anesthesia Neurological disorders
- 19. Autoscopic psychosis The experience in which an individual perceives the surrounding environment from a different perspective,
- 20. Migraine with Aura Micropsy Macropsy Distortions Flashes Geometrical shapes
- 21. Hypnagogic/ Hypnapompic Hallucinations Only upon falling asleep/ waking up Very common Normal phenomenon! Seconds to minutes
- 22. Illusions Unrealistic interpretation of realistic stimulus Normal! Common in the dark
- 23. הזיות Substance- Induced Visual Experiences Hallucinogens Intoxication- stimulants, cocaine, alcohol Withdrawal- alcohol, BZ
- 24. Delirium Tremens
- 25. Treatment Options ORGANICALLY BASED HALLUCINATIONS ARE USUALLY SELF-LIMITING. With either end organ or central nervous system
- 26. Delusions False belief, based on the incorrect interpretation of the external reality, not in cultural context,
- 27. Types of Delusions Paranoid/persecutory Ideas of reference External locus of control Thought broadcasting Thought insertion, withdrawal
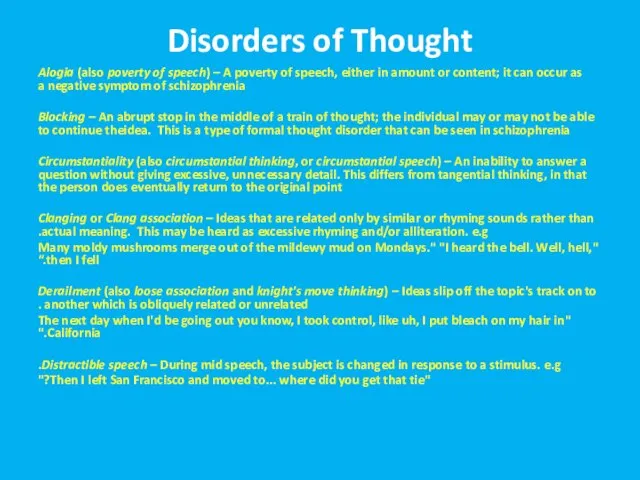
- 28. Disorders of Thought Alogia (also poverty of speech) – A poverty of speech, either in amount
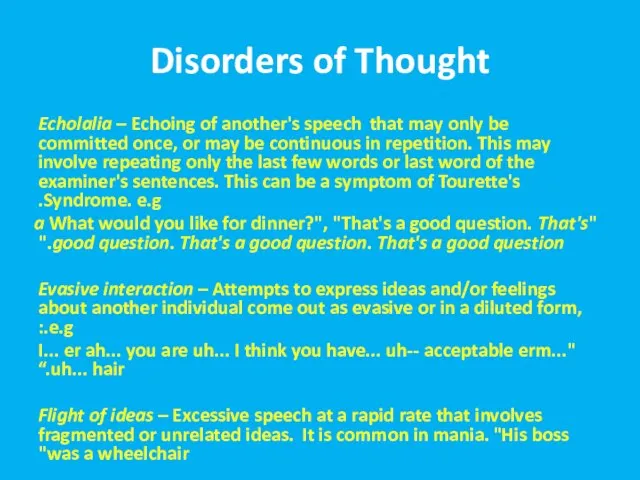
- 29. Disorders of Thought Echolalia – Echoing of another's speech that may only be committed once, or
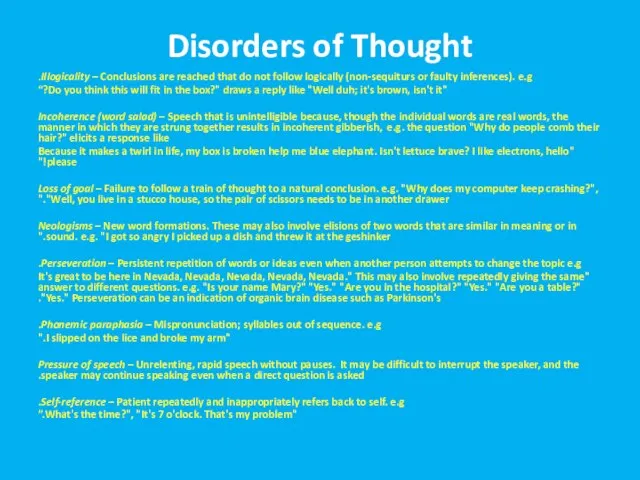
- 30. Disorders of Thought Illogicality – Conclusions are reached that do not follow logically (non-sequiturs or faulty
- 31. Disorders of Thought Semantic paraphasia – Substitution of inappropriate word. e.g. "I slipped on the coat,
- 32. Behavior Bizarre dress and appearance Catatonia Loss of impulse control Aggression and extreme irritability Stereotypic speech
- 33. Catatonia Stupor (i.e., no psychomotor activity; not actively relating to environment) Catalepsy (i.e., passive induction of
- 34. Mood and Affect Inappropriate affect Blunting of affect/mood
- 35. מצב פסיכוטי פרנואידי- הדגמה Movie
- 36. DDX Basis- primary versus secondary psychosis!
- 37. DDX- Primary Psychosis Schizophrenia, schizophreniform Schizoaffective Brief Psychotic disorder Delusional disorder Affective psychosis (depression, mania)
- 38. DDX- Secondary Psychosis Substance/ Medication- induced Psychosis secondary to another medical condition (neurological, endocrinological, metabolic, infectious)
- 39. Workup- Always Rule Out Secondary Cause!"אורגנית" Good anamnesys Thorough physical and neurological exam Lab and imaging:
- 40. Secondary Psychotic Disorders Psychotic Disorder due to Another Medical Condition Substance Induced Psychotic Disorder Delirium Dementia
- 41. Psychotic Disorder due to Another Medical Condition Prominent hallucinations or delusions There is evidence from the
- 42. Psychotic Disorder due to Another Medical Condition Neurological conditions (e.g., neoplasms, cerebrovascular disease, Huntington's disease, multiple
- 45. Over the counter: Dextromethorphan, cold medications Other: Steroids, Bupropion, Dostinex, antibiotics, antivirals, antimalarials
- 47. Delirium 15-25% of patients on general medical wards, S/P surgery- even higher percentages Advanced age, any
- 48. Delirium Perceptual disturbances are common; however, hallucinations also are frequent: Hallucinations: 40% to 67% Delusions: 25%
- 49. Etiologies In general- delirium etiology =secondary psychosis etiology! Intracranial Causes: Seizures and Postictal states Brain Trauma
- 50. Etiologies cont’d Extracranial causes: Drugs/Medications- toxicity, intoxication, and w/d. Poisons (Carbon Monoxide, Heavy metals) Endocrine dysfunction
- 51. Etiologies cont’d Systemic Infections Electrolyte abnormalities Postoperative states Trauma
- 52. Treatment of Delirium High Potency Antipsychotic+ antihistamine Supportive Care Find and Resolve Causative Factor(s)
- 53. Dementia as the Cause of Psychosis
- 54. DSM-IV criteria for the diagnosis of Dementia of the Alzheimer's Type A. The development of multiple
- 55. Alzheimer’s Disease Prevalence of psychotic symptoms: 16% to 70%; Median: 37% for delusions; 4% to 76%
- 56. Vascular Dementia Cache County study found prevalence of hallucinations similar between AD and VaD, but delusions
- 57. Lewy Body Dementia About half have visual hallucinations (up to 80% in some studies), and it’s
- 58. Parkinson’s disease Overall rates: 20 to 60% --- about ¼ have hallucinations in PD, but ¾
- 59. Test Yourself
- 60. Symptoms of secondary psychoses accompany which disorder: 1. Delusional disorder 2. Schizophrenia 3. Depression 4. Alzheimer’s
- 61. In delirium, what is the most common form of hallucinations? 1. Auditory 2. Tactile 3. Visual
- 62. In Alzheimer’s disease which of the following is true : 1. Auditory hallucinations are the most
- 63. In Parkinson’s disease which of the following is true: 1. Extrinsic causes of hallucinations are greater
- 65. Скачать презентацию
מבנה ההרצאה
What is Psychosis?
Symptoms
DDX
מבנה ההרצאה
What is Psychosis?
Symptoms
DDX
Psychosis
Inability to distinguish between the reality and the inner world and
Psychosis
Inability to distinguish between the reality and the inner world and
Why does it happen?
Dopaminergic Theory
Increasing levels of dopamine in the brain
Why does it happen?
Dopaminergic Theory
Increasing levels of dopamine in the brain
סימפטומים
Signs of psychosis
Hallucinations
Delusions
Bizarre or disorganized behavior
Impaired thought process
Impaired speech output
Abnormal movements
סימפטומים
Signs of psychosis
Hallucinations
Delusions
Bizarre or disorganized behavior
Impaired thought process
Impaired speech output
Abnormal movements
הזיוHallucinationsת
Abnormal perceptional experience unrelated to external stimuli
5 senses
הזיוHallucinationsת
Abnormal perceptional experience unrelated to external stimuli
5 senses
Reasons for Hallucinations
Primary psychiatric disorders
Brain pathology
Substances
Disorders of cranial nerves
Delirium
Dementia
Reasons for Hallucinations
Primary psychiatric disorders
Brain pathology
Substances
Disorders of cranial nerves
Delirium
Dementia
Auditory Hallucinations
Primary psychotic disorders- human voices, noises, command hallucinations. Usually perceived
Auditory Hallucinations
Primary psychotic disorders- human voices, noises, command hallucinations. Usually perceived
Taste Hallucinations
Usually epilepsy and brain pathology
Very rare in primary psychiatric disorders
Do
Taste Hallucinations
Usually epilepsy and brain pathology
Very rare in primary psychiatric disorders
Do
Smell Hallucinations
Usually epilepsy and brain pathology
Rare in primary psychiatric disorders- possible
Smell Hallucinations
Usually epilepsy and brain pathology
Rare in primary psychiatric disorders- possible
Somatic and Tactile Hallucinations
Usually epilepsy and brain pathology
In primary psychiatric disorders-
Somatic and Tactile Hallucinations
Usually epilepsy and brain pathology
In primary psychiatric disorders-
Visual Hallucinations
Usually epilepsy and brain pathology, migraines, visual impairment
In primary psychiatric
Visual Hallucinations
Usually epilepsy and brain pathology, migraines, visual impairment
In primary psychiatric
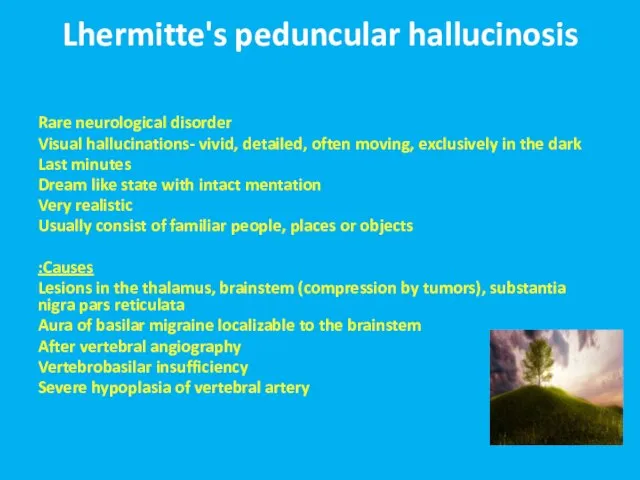
Lhermitte's peduncular hallucinosis
Rare neurological disorder
Visual hallucinations- vivid, detailed, often moving, exclusively
Lhermitte's peduncular hallucinosis
Rare neurological disorder
Visual hallucinations- vivid, detailed, often moving, exclusively
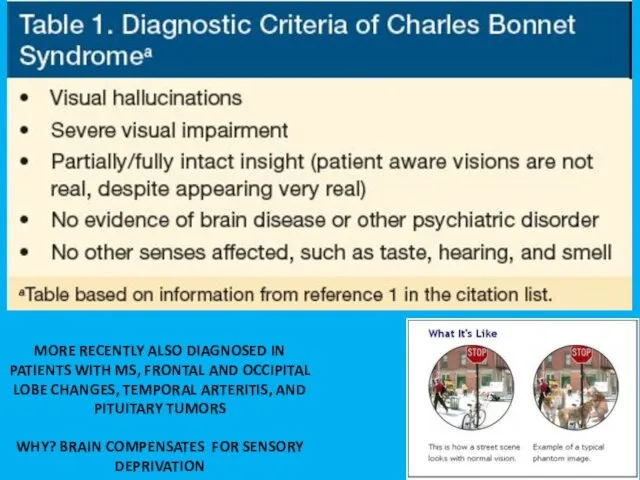
MORE RECENTLY ALSO DIAGNOSED IN PATIENTS WITH MS, FRONTAL AND OCCIPITAL
MORE RECENTLY ALSO DIAGNOSED IN PATIENTS WITH MS, FRONTAL AND OCCIPITAL
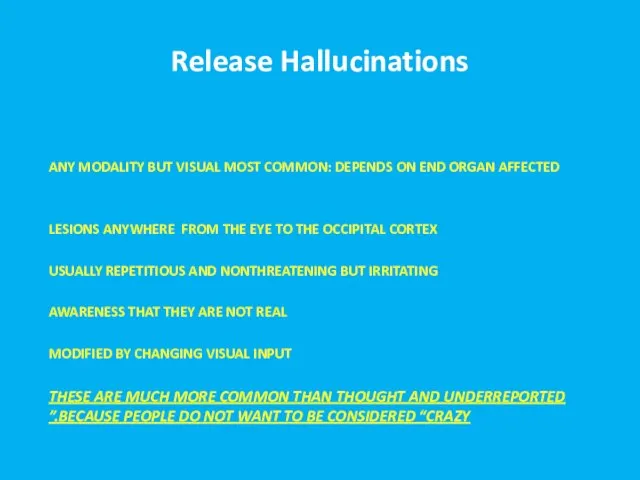
Release Hallucinations
ANY MODALITY BUT VISUAL MOST COMMON: DEPENDS ON END ORGAN
Release Hallucinations
ANY MODALITY BUT VISUAL MOST COMMON: DEPENDS ON END ORGAN
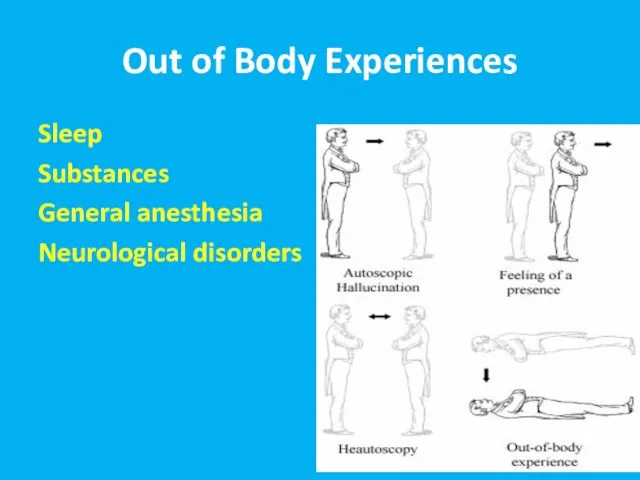
Out of Body Experiences
Sleep
Substances
General anesthesia
Neurological disorders
Out of Body Experiences
Sleep
Substances
General anesthesia
Neurological disorders
Autoscopic psychosis
The experience in which an individual perceives the surrounding environment
Autoscopic psychosis
The experience in which an individual perceives the surrounding environment
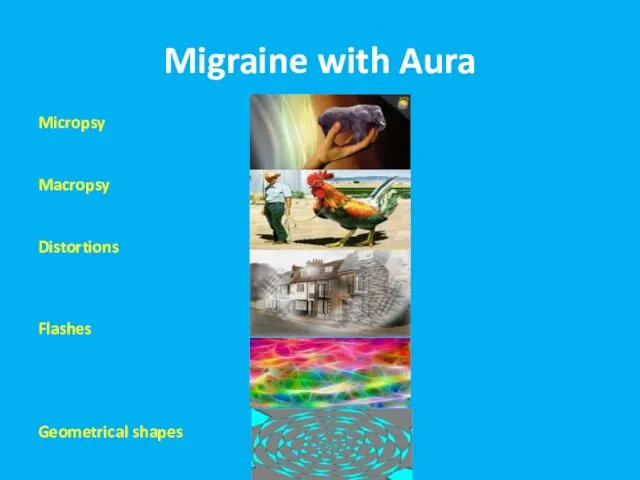
Migraine with Aura
Micropsy
Macropsy
Distortions
Flashes
Geometrical shapes
Migraine with Aura
Micropsy
Macropsy
Distortions
Flashes
Geometrical shapes
Hypnagogic/ Hypnapompic Hallucinations
Only upon falling asleep/ waking up
Very common
Normal phenomenon!
Seconds to
Hypnagogic/ Hypnapompic Hallucinations
Only upon falling asleep/ waking up
Very common
Normal phenomenon!
Seconds to
Illusions
Unrealistic interpretation of realistic stimulus
Normal!
Common in the dark
Illusions
Unrealistic interpretation of realistic stimulus
Normal!
Common in the dark
הזיות Substance- Induced Visual Experiences
Hallucinogens
Intoxication- stimulants, cocaine, alcohol
Withdrawal- alcohol, BZ
הזיות Substance- Induced Visual Experiences
Hallucinogens
Intoxication- stimulants, cocaine, alcohol
Withdrawal- alcohol, BZ
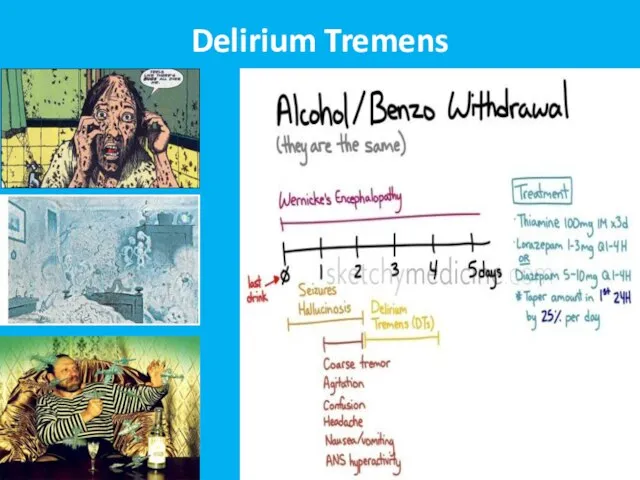
Delirium Tremens
Delirium Tremens

Treatment Options
ORGANICALLY BASED HALLUCINATIONS ARE USUALLY SELF-LIMITING. With either end organ
Treatment Options
ORGANICALLY BASED HALLUCINATIONS ARE USUALLY SELF-LIMITING. With either end organ
Delusions
False belief, based on the incorrect interpretation of the external reality,
Delusions
False belief, based on the incorrect interpretation of the external reality,
Types of Delusions
Paranoid/persecutory
Ideas of reference
External locus of control
Thought broadcasting
Thought insertion,
Types of Delusions
Paranoid/persecutory
Ideas of reference
External locus of control
Thought broadcasting
Thought insertion,
Disorders of Thought
Alogia (also poverty of speech) – A poverty of speech, either in
Disorders of Thought
Alogia (also poverty of speech) – A poverty of speech, either in
Disorders of Thought
Echolalia – Echoing of another's speech that may only be
Disorders of Thought
Echolalia – Echoing of another's speech that may only be
Disorders of Thought
Illogicality – Conclusions are reached that do not follow logically
Disorders of Thought
Illogicality – Conclusions are reached that do not follow logically
Disorders of Thought
Semantic paraphasia – Substitution of inappropriate word. e.g.
"I slipped on
Disorders of Thought
Semantic paraphasia – Substitution of inappropriate word. e.g.
"I slipped on
Behavior
Bizarre dress and appearance
Catatonia
Loss of impulse control
Aggression and extreme irritability
Stereotypic speech
Behavior
Bizarre dress and appearance
Catatonia
Loss of impulse control
Aggression and extreme irritability
Stereotypic speech
Catatonia
Stupor (i.e., no psychomotor activity; not actively relating to environment)
Catalepsy (i.e., passive induction
Catatonia
Stupor (i.e., no psychomotor activity; not actively relating to environment)
Catalepsy (i.e., passive induction
Mood and Affect
Inappropriate affect
Blunting of affect/mood
Mood and Affect
Inappropriate affect
Blunting of affect/mood
מצב פסיכוטי פרנואידי- הדגמה
Movie
מצב פסיכוטי פרנואידי- הדגמה
Movie
DDX
Basis- primary versus secondary psychosis!
DDX
Basis- primary versus secondary psychosis!
DDX- Primary Psychosis
Schizophrenia, schizophreniform
Schizoaffective
Brief Psychotic disorder
Delusional disorder
Affective psychosis (depression, mania)
DDX- Primary Psychosis
Schizophrenia, schizophreniform
Schizoaffective
Brief Psychotic disorder
Delusional disorder
Affective psychosis (depression, mania)
DDX- Secondary Psychosis
Substance/ Medication- induced
Psychosis secondary to another medical condition (neurological,
DDX- Secondary Psychosis
Substance/ Medication- induced
Psychosis secondary to another medical condition (neurological,
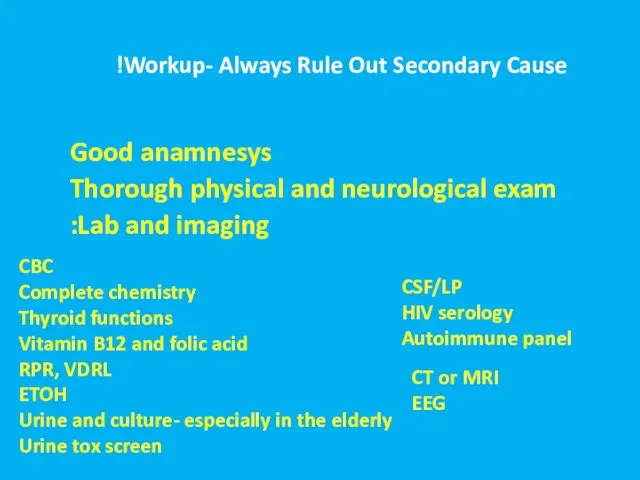
Workup- Always Rule Out Secondary Cause!"אורגנית"
Good anamnesys
Thorough physical and
Workup- Always Rule Out Secondary Cause!"אורגנית"
Good anamnesys
Thorough physical and
Secondary Psychotic Disorders
Psychotic Disorder due to Another Medical Condition
Substance Induced Psychotic
Secondary Psychotic Disorders
Psychotic Disorder due to Another Medical Condition
Substance Induced Psychotic
Psychotic Disorder due to Another Medical Condition
Prominent hallucinations or delusions
There is
Psychotic Disorder due to Another Medical Condition
Prominent hallucinations or delusions
There is
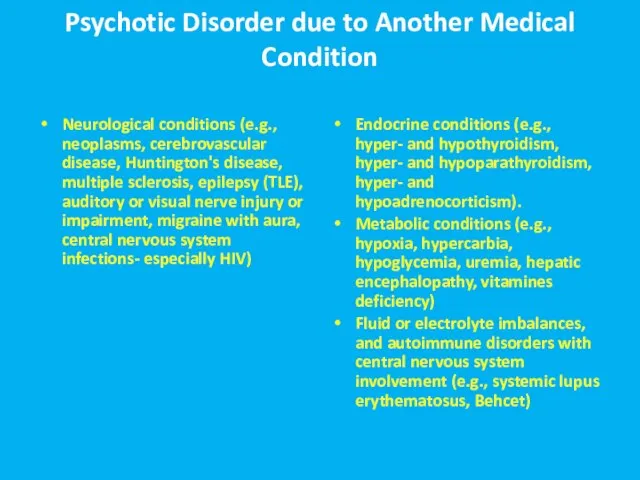
Psychotic Disorder due to Another Medical Condition
Neurological conditions (e.g., neoplasms, cerebrovascular
Psychotic Disorder due to Another Medical Condition
Neurological conditions (e.g., neoplasms, cerebrovascular
Over the counter: Dextromethorphan, cold medications
Other: Steroids, Bupropion, Dostinex, antibiotics, antivirals,
Over the counter: Dextromethorphan, cold medications
Other: Steroids, Bupropion, Dostinex, antibiotics, antivirals,
Delirium
15-25% of patients on general medical wards, S/P surgery- even higher
Delirium
15-25% of patients on general medical wards, S/P surgery- even higher
Delirium
Perceptual disturbances are common; however, hallucinations also are frequent:
Hallucinations:
Delirium
Perceptual disturbances are common; however, hallucinations also are frequent:
Hallucinations:
Etiologies
In general- delirium etiology =secondary psychosis etiology!
Intracranial Causes: Seizures and Postictal
Etiologies
In general- delirium etiology =secondary psychosis etiology!
Intracranial Causes: Seizures and Postictal
Etiologies cont’d
Extracranial causes: Drugs/Medications- toxicity, intoxication, and w/d.
Poisons (Carbon Monoxide,
Etiologies cont’d
Extracranial causes: Drugs/Medications- toxicity, intoxication, and w/d.
Poisons (Carbon Monoxide,
Etiologies cont’d
Systemic Infections
Electrolyte abnormalities
Postoperative states
Trauma
Etiologies cont’d
Systemic Infections
Electrolyte abnormalities
Postoperative states
Trauma
Treatment of Delirium
High Potency Antipsychotic+ antihistamine
Supportive Care
Find and Resolve Causative Factor(s)
Treatment of Delirium
High Potency Antipsychotic+ antihistamine
Supportive Care
Find and Resolve Causative Factor(s)
Dementia as the Cause of Psychosis
Dementia as the Cause of Psychosis
DSM-IV criteria for the diagnosis of Dementia of the Alzheimer's Type
A.
DSM-IV criteria for the diagnosis of Dementia of the Alzheimer's Type
A.
Alzheimer’s Disease
Prevalence of psychotic symptoms: 16% to 70%; Median: 37% for
Alzheimer’s Disease
Prevalence of psychotic symptoms: 16% to 70%; Median: 37% for
Vascular Dementia
Cache County study found prevalence of hallucinations similar between
Vascular Dementia
Cache County study found prevalence of hallucinations similar between
Lewy Body Dementia
About half have visual hallucinations (up to 80% in
Lewy Body Dementia
About half have visual hallucinations (up to 80% in
Parkinson’s disease
Overall rates: 20 to 60% --- about ¼ have
Parkinson’s disease
Overall rates: 20 to 60% --- about ¼ have
Test Yourself
Test Yourself
Symptoms of secondary psychoses accompany which disorder:
1. Delusional disorder
2. Schizophrenia
3.
Symptoms of secondary psychoses accompany which disorder:
1. Delusional disorder
2. Schizophrenia
3.
In delirium, what is the most common form of hallucinations?
1. Auditory
2.
In delirium, what is the most common form of hallucinations?
1. Auditory
2.
In Alzheimer’s disease which of the following is true :
1. Auditory
In Alzheimer’s disease which of the following is true :
1. Auditory
In Parkinson’s disease which of the following is true:
1. Extrinsic causes
In Parkinson’s disease which of the following is true:
1. Extrinsic causes
 Тест Люшера
Тест Люшера Закономерности психического развития
Закономерности психического развития Гестози вагітних
Гестози вагітних Типы темперамента. Тест
Типы темперамента. Тест Восприятие детей с задержкой психического развития (ЗПР)
Восприятие детей с задержкой психического развития (ЗПР) Неалкогольная жировая болезнь печени
Неалкогольная жировая болезнь печени Наследственные аномалии с нарушением прикуса
Наследственные аномалии с нарушением прикуса Презентация по медицине Эндогенные интоксикации в хирургии и принципы их коррекции
Презентация по медицине Эндогенные интоксикации в хирургии и принципы их коррекции  Лекарственные средства, влияющие на артериальное давление
Лекарственные средства, влияющие на артериальное давление SIW “Nasal bleeding tamponade”
SIW “Nasal bleeding tamponade” Кора головного мозга. Высшие мозговые функции и их расстройства
Кора головного мозга. Высшие мозговые функции и их расстройства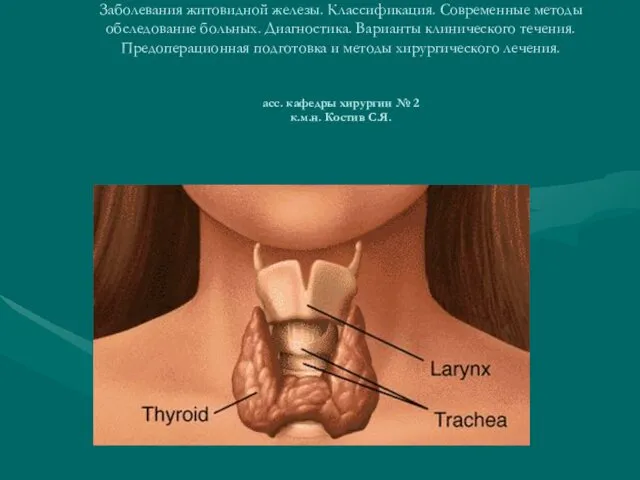 Заболевания щитовидной железы. Классификация. Современные методы обследование больных. Диагностика
Заболевания щитовидной железы. Классификация. Современные методы обследование больных. Диагностика Периоперативная безопасность пациента
Периоперативная безопасность пациента Иммунды жүйенің құрылысы. Антигендер
Иммунды жүйенің құрылысы. Антигендер Презентация по медицине Острая анаэробная инфекция. Госпитальная инфекция
Презентация по медицине Острая анаэробная инфекция. Госпитальная инфекция  Медицинская паразитология. Паразитические простейшие
Медицинская паразитология. Паразитические простейшие Количественная эхокардиография. (Лекция 3)
Количественная эхокардиография. (Лекция 3) Доказанная инволюция фиброза печени
Доказанная инволюция фиброза печени Московский государственный университет. Его роль в развитии медицины
Московский государственный университет. Его роль в развитии медицины Патофизиология мочекаменной болезни
Патофизиология мочекаменной болезни Методы исследования мочевыделительной системы
Методы исследования мочевыделительной системы Клиническая интерпретация анализа крови у детей
Клиническая интерпретация анализа крови у детей Красная волчанка
Красная волчанка Меню на день для пациента с метаболическим синдромом
Меню на день для пациента с метаболическим синдромом Анатомия для массажистов
Анатомия для массажистов СРС. Клинический случай пациента с синдромом лимфоаденопатии
СРС. Клинический случай пациента с синдромом лимфоаденопатии Транзиторная ишемическая атака. Этиология. Патогенез. Клиника
Транзиторная ишемическая атака. Этиология. Патогенез. Клиника Остеоартроз. Введение в проблему
Остеоартроз. Введение в проблему