- Schonlein - Hennoch purpura

Содержание
- 2. Henoch-Schönlein Purpura (HSP) is a common vasculitis of small vessels with cutaneous and systemic complications. It
- 3. EPIDEMIOLOGY The etiology is unknown more frequent in children than adults, with most cases occurring between
- 4. PATHOGENESIS in specific populations, patients with HSP have a significantly higher frequency of HLA-DRB1*01 and decreased
- 5. CTLA-4 +49 A/G genotype and HLA-DRB1 polymorphisms in Turkish patients with Henoch-Schönlein purpura. presence of Cytotoxic
- 7. The immunobiology of Henoch-Schönlein purpura. group A beta-hemolytic streptococcus (GAS) has widely studied and found in
- 8. CLINICAL MANIFESTATIONS The disease onset may be acute, or insidious, with sequential occurrence of symptoms over
- 9. CLINICAL MANIFESTATIONS Rash (95-100%), especially involving the legs, may not be present on initial presentation Subcutaneous
- 10. Rash beginning as pinkish maculopapules that initially blanch on pressure and progress to petechiae or purpura,
- 11. Rash
- 12. Arthritis present in more than ⅔ of children with HSP, is usually localized to the knees
- 13. Gastrointestinal tract intermittent abdominal pain that is often colicky in nature. There may be peritoneal exudate,
- 14. Renal involvement occurs in 25-50% of children may manifest with: hematuria, proteinuria, or both; nephritis or
- 15. Increased serum levels of insulin-like growth factor (IGF)-1 and IGF-binding protein-3 in Henoch-Schonlein purpura. Serum IGF-1
- 16. What is the difference between IgA nephropathy and Henoch-Schönlein purpura nephritis
- 17. Relationship between initial clinical signs and risk of chronic renal failure in Henoch-Schönlein purpura nephritis
- 18. Complications of Henoch-Schönlein Purpura Hepatosplenomegaly Myocardial infarction Pulmonary hemorrhage Pleural effusion Unnecessary abdominal surgery Intussusception Hemorrhage
- 19. DIAGNOSIS Diagnostic uncertainty arises when the symptom complex of edema, rash, arthritis with abdominal complaints, and
- 20. DIAGNOSIS Affected children often have a moderate thrombocytosis and leukocytosis. The erythrocyte sedimentation rate (ESR) may
- 21. Definitive diagnosis confirmed by biopsy cutaneous site showing leukocytoclastic angiitis. Renal biopsy may show mesangial deposition
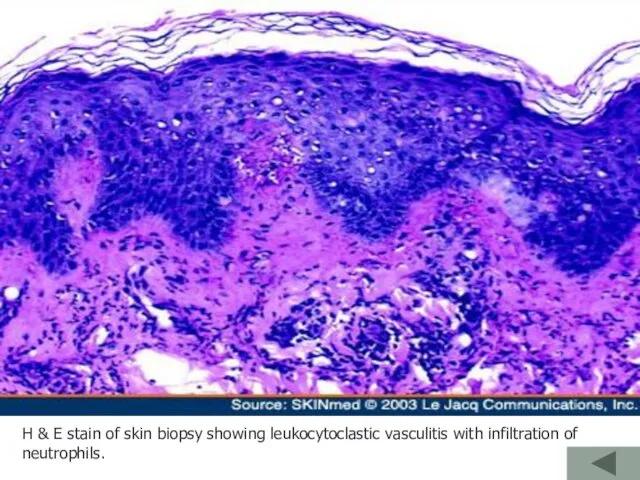
- 22. H & E stain of skin biopsy showing leukocytoclastic vasculitis with infiltration of neutrophils.
- 23. Henoch-Schönlein purpura. A: Cutaneous purpura; B: Urine sediment red blood cell cast; C: Acute glomerular inflammation
- 24. Immunofluorescence micrograph of a glomerulus from a patient with HSP nephropathy stained for the presence of
- 25. Differential Diagnosis of Henoch-Schönlein Purpura Acute abdomen Meningococcal meningitis or septicemia Rheumatoid arthritis Rheumatic fever Idiopathic
- 26. Acute hemorrhagic edema (AHE) is an acute cutaneous benign leukocytoclastic vasculitis seen in children ≤2 yr
- 27. Acute hemorrhagic edema (AHE)
- 28. TREATMENT Symptomatic treatment adequate hydration, bland diet, pain control with acetaminophen is provided for self-limited complaints
- 29. TREATMENT Therapy with oral or intravenous corticosteroids (1-2 mg/kg/day) is often associated with dramatic improvement of
- 30. TREATMENT is the same as for other forms of acute glomerulonephritis If anti-cardiolipin or antiphospholipid antibodies
- 31. Prognosis More than 80% of patients have a single isolated episode lasting a few weeks. Approximately
- 33. Скачать презентацию
Henoch-Schönlein Purpura (HSP)
is a common vasculitis of small vessels with
Henoch-Schönlein Purpura (HSP)
is a common vasculitis of small vessels with
EPIDEMIOLOGY
The etiology is unknown
more frequent in children than adults, with most
EPIDEMIOLOGY
The etiology is unknown
more frequent in children than adults, with most
PATHOGENESIS
in specific populations, patients with HSP have a significantly higher
PATHOGENESIS
in specific populations, patients with HSP have a significantly higher
CTLA-4 +49 A/G genotype and HLA-DRB1 polymorphisms in Turkish patients with
CTLA-4 +49 A/G genotype and HLA-DRB1 polymorphisms in Turkish patients with
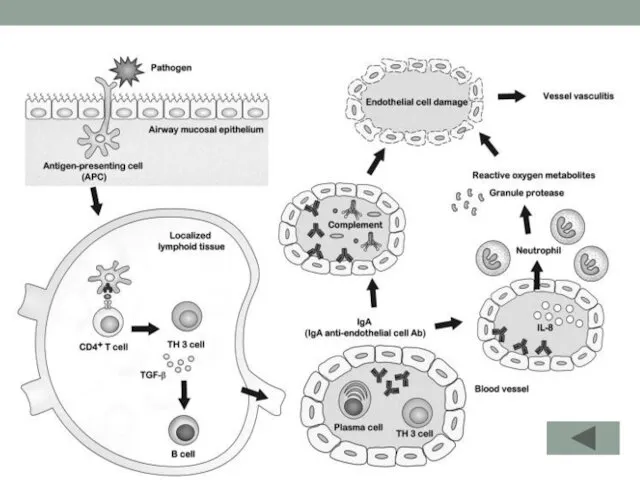
The immunobiology of Henoch-Schönlein purpura.
group A beta-hemolytic streptococcus (GAS) has widely
The immunobiology of Henoch-Schönlein purpura.
group A beta-hemolytic streptococcus (GAS) has widely
CLINICAL MANIFESTATIONS
The disease onset may be acute, or insidious, with sequential
CLINICAL MANIFESTATIONS
The disease onset may be acute, or insidious, with sequential
CLINICAL MANIFESTATIONS
Rash (95-100%), especially involving the legs, may not be present
CLINICAL MANIFESTATIONS
Rash (95-100%), especially involving the legs, may not be present
Rash
beginning as pinkish maculopapules that initially blanch on pressure and
Rash
beginning as pinkish maculopapules that initially blanch on pressure and

Rash
Rash
Arthritis
present in more than ⅔ of children with HSP,
is usually
Arthritis
present in more than ⅔ of children with HSP,
is usually
Gastrointestinal tract
intermittent abdominal pain that is often colicky in nature.
There
Gastrointestinal tract
intermittent abdominal pain that is often colicky in nature.
There
Renal involvement
occurs in 25-50% of children
may manifest with:
hematuria,
proteinuria, or
Renal involvement
occurs in 25-50% of children
may manifest with:
hematuria,
proteinuria, or
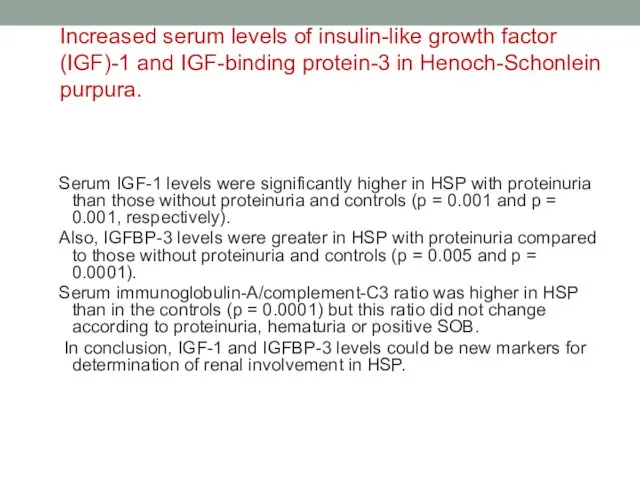
Increased serum levels of insulin-like growth factor (IGF)-1 and IGF-binding protein-3
Increased serum levels of insulin-like growth factor (IGF)-1 and IGF-binding protein-3
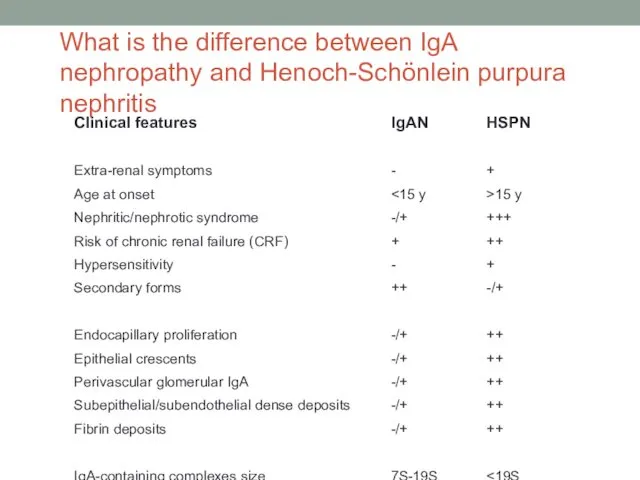
What is the difference between IgA nephropathy and Henoch-Schönlein purpura nephritis
What is the difference between IgA nephropathy and Henoch-Schönlein purpura nephritis
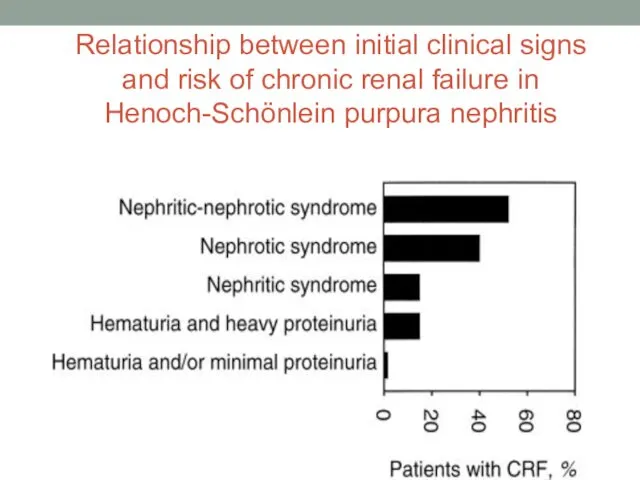
Relationship between initial clinical signs and risk of chronic renal failure
Relationship between initial clinical signs and risk of chronic renal failure
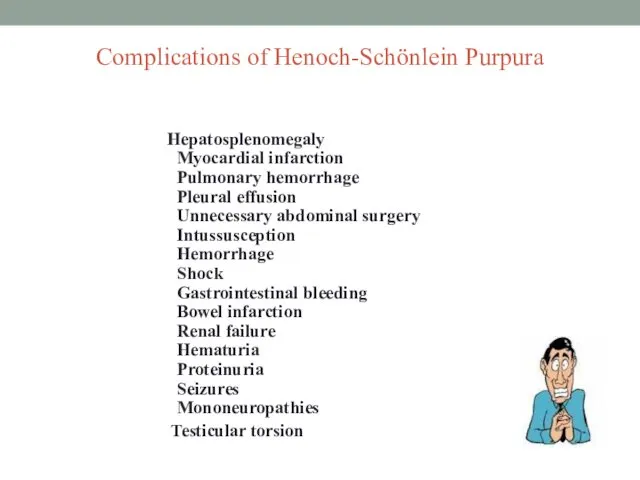
Complications of Henoch-Schönlein Purpura
Hepatosplenomegaly
Myocardial infarction
Pulmonary hemorrhage
Pleural
Complications of Henoch-Schönlein Purpura
Hepatosplenomegaly Myocardial infarction Pulmonary hemorrhage Pleural
DIAGNOSIS
Diagnostic uncertainty arises when the symptom complex of edema, rash, arthritis
DIAGNOSIS
Diagnostic uncertainty arises when the symptom complex of edema, rash, arthritis
DIAGNOSIS
Affected children often have a moderate thrombocytosis and leukocytosis.
The erythrocyte
DIAGNOSIS
Affected children often have a moderate thrombocytosis and leukocytosis.
The erythrocyte
Definitive diagnosis confirmed by biopsy
cutaneous site showing leukocytoclastic angiitis.
Renal biopsy
Definitive diagnosis confirmed by biopsy
cutaneous site showing leukocytoclastic angiitis.
Renal biopsy
H & E stain of skin biopsy showing leukocytoclastic vasculitis with
H & E stain of skin biopsy showing leukocytoclastic vasculitis with
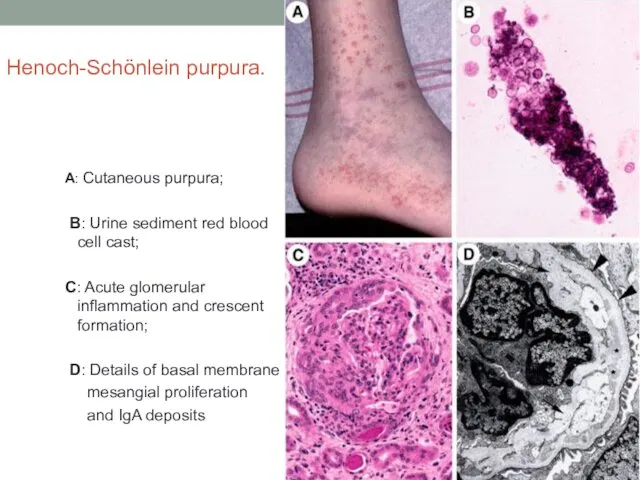
Henoch-Schönlein purpura.
A: Cutaneous purpura;
B: Urine sediment red blood cell
Henoch-Schönlein purpura.
A: Cutaneous purpura;
B: Urine sediment red blood cell
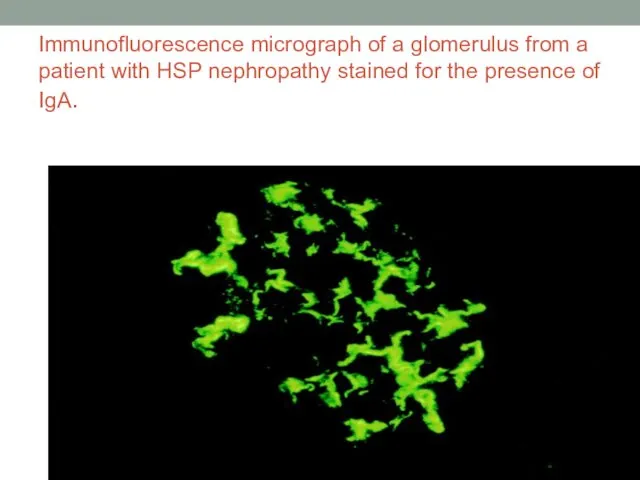
Immunofluorescence micrograph of a glomerulus from a patient with HSP nephropathy
Immunofluorescence micrograph of a glomerulus from a patient with HSP nephropathy
Differential Diagnosis of Henoch-Schönlein Purpura
Acute abdomen
Meningococcal meningitis or septicemia
Rheumatoid
Differential Diagnosis of Henoch-Schönlein Purpura
Acute abdomen
Meningococcal meningitis or septicemia
Rheumatoid
Acute hemorrhagic edema (AHE)
is an acute cutaneous benign leukocytoclastic vasculitis
seen
Acute hemorrhagic edema (AHE)
is an acute cutaneous benign leukocytoclastic vasculitis
seen

Acute hemorrhagic edema (AHE)
Acute hemorrhagic edema (AHE)
TREATMENT
Symptomatic treatment
adequate hydration,
bland diet,
pain control with acetaminophen is
TREATMENT
Symptomatic treatment
adequate hydration,
bland diet,
pain control with acetaminophen is
TREATMENT
Therapy with oral or intravenous corticosteroids (1-2 mg/kg/day) is often associated
TREATMENT
Therapy with oral or intravenous corticosteroids (1-2 mg/kg/day) is often associated
TREATMENT
is the same as for other forms of acute glomerulonephritis
If
TREATMENT
is the same as for other forms of acute glomerulonephritis
If
Prognosis
More than 80% of patients have a single isolated episode lasting
Prognosis
More than 80% of patients have a single isolated episode lasting
 Отклонение в интеллектуальном развитии у детей
Отклонение в интеллектуальном развитии у детей Кожный шов
Кожный шов Спілкування – це процес встановлення і розвитку контакту між людьми. Лекція №4
Спілкування – це процес встановлення і розвитку контакту між людьми. Лекція №4 Физиология системы выделения. Функции почек. Механизмы мочеобразования
Физиология системы выделения. Функции почек. Механизмы мочеобразования Возбудитель сибирской язвы
Возбудитель сибирской язвы Сахарный диабет
Сахарный диабет Гинекологиялық операциялардан кейінгі науқастардың тамақтануы
Гинекологиялық операциялардан кейінгі науқастардың тамақтануы Задачи, организационная структура и основы деятельности Всероссийской службы медицины катастроф
Задачи, организационная структура и основы деятельности Всероссийской службы медицины катастроф Практикум по методам психологического исследования. Лабораторное занятие № 1
Практикум по методам психологического исследования. Лабораторное занятие № 1 Наркотики
Наркотики Гигиена кожи
Гигиена кожи Охрана зрения слабовидящего дошкольника
Охрана зрения слабовидящего дошкольника Врачевание на средневековом востоке
Врачевание на средневековом востоке Медична гельмінтологія. Плоскі та круглі черви паразити людини
Медична гельмінтологія. Плоскі та круглі черви паразити людини Франшиза: медицинский центр профилактики
Франшиза: медицинский центр профилактики Множественная лекарственная устойчивость МБТ
Множественная лекарственная устойчивость МБТ Уход за больными с повреждениями позвоночника, спинного мозга, таза
Уход за больными с повреждениями позвоночника, спинного мозга, таза Инсульт. Статистика инсульта
Инсульт. Статистика инсульта Человек и его здоровье. Кровь. Кровообращение
Человек и его здоровье. Кровь. Кровообращение Стандартизация в медицине и здравоохранении
Стандартизация в медицине и здравоохранении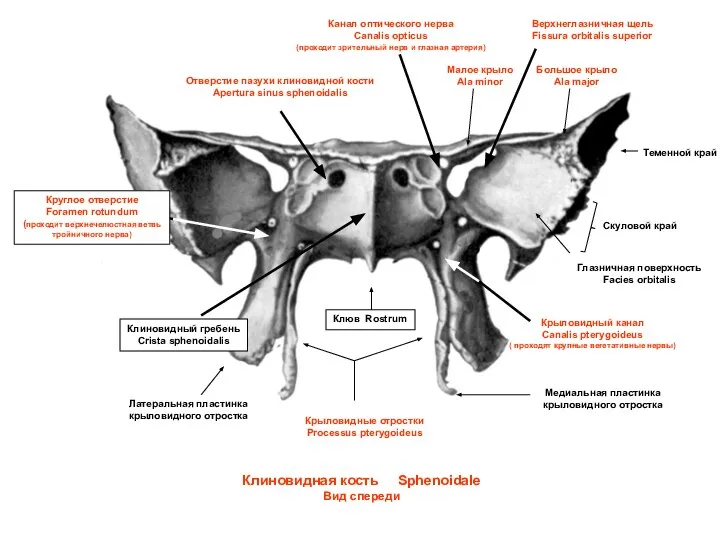 Клиновидная кость. Вид спереди
Клиновидная кость. Вид спереди Инсульттер кезіндегі алғашқы көмек алгоритмі
Инсульттер кезіндегі алғашқы көмек алгоритмі Медико-социальные аспекты демографии
Медико-социальные аспекты демографии Аттестационная работа. Влияние на организм младшего школьника компьютерных и подвижных игр
Аттестационная работа. Влияние на организм младшего школьника компьютерных и подвижных игр Гостра ревматична лихоманка у дітей
Гостра ревматична лихоманка у дітей Потапова А.С
Потапова А.С Некротическая флегмона новорожденных
Некротическая флегмона новорожденных Основы доказательной медицины
Основы доказательной медицины